
|
1 Comment
Many managers, supervisors and leads say that safety leaders are made, not born. Though when I think about effective safety champions I have known over the years, I realize that most started on the factory floor or in the trades and transitioned into the safety field after many years in their organization. Others were passionate about a single issue and took steps to address it and then went back to their functional job. Most become key members of a Safety Committee or Tiger Team and exercise informal leadership across their companies to improve safety and working conditions. Any way you slice it, informal safety leaders can make meaningful changes within their organizations. Let’s think about what it takes to be a leader in any line of work:
Most smart organizations look for potential safety leaders among the experienced workers in the skilled trades or from the shop floor because those people have the credibility to be taken seriously by the rest of the workforce. These individuals are already influencers of their fellow workers, and provide a bridge between workers and management in all areas of the work. Effective informal leaders don’t have a job title or the authority of a management position, but they influence others with their confidence, personality and credibility. Identifying potential safety leaders by involving workers who already have the skills and traits discussed above has proven more successful than selecting employees by seniority (long term or short!) and putting them through safety training or advanced communications classes. Since much of the motivation for leadership comes from within an individual, safety leaders, like other leaders who shape organizations, are born not made. A client recently contacted me to ask for a straightforward yet effective method of post-incident root cause analysis. Like many companies, their process had devolved into a blame-game in which the "root causes" in various incidents all came back to employee behavior or "not paying attention". Consequently, the corrective actions "retraining" and "presenting lessons learned" were not preventing similar incidents from happening. No surprise there... On the other hand, the company is small and they didn't want an over-complicated process that would require alot of up-front training to deploy. This process is based on the "Hazard-Barrier-Target Analysis" method, plus 2 of the famous "5-Whys". A Hazard-Barrier-Target Analysis (Hazard-BTA) process begins with describing the incident, examines how damage occurs, and assesses the adequacy of installed barriers or other safeguards that should either prevent or mitigate an incident. For a damage-causing incident to occur, there must be a target (what is affected), a hazard and less-than-adequate barriers. By identifying possible targets, barriers can be analyzed. A target is something of value; it may be a person, part, equipment, system, procedure or process. A barrier separates the target from the hazard and may be physical (such as personal protective equipment, machine guards or safety valves), administrative (procedures or directives) or personal (employee training and supervision) (Wilson, et al 133). To determine causation, a simple process of determining why the barrier failed or was inadequate will allow us to drill down past the obvious direct causes (like employees doing the wrong thing) to the systemic (root) causes of failure such as improper procedures, poor employee training, lack of resources provided by the company, etc. The goal of this process is to determine actionable corrective actions which will reinforce or replace the deficient barriers and actually prevent a similar occurrence from happening in the future. EXAMPLE: Two chemical plant employees were opening a process line at a flange joint in order to unclog the line. As the line was opened, the clog shifted, causing the product inside the line to splash the workers. As a result, each suffered multiple second and third-degree burns. In this case, a hazard-BTA (Table below) proved to be an efficient assessment tool that provided valuable information in a relatively short period of time. PROCEDURE:
CORRECTIVE ACTIONS: This process results in determining concrete corrective actions that are not punitive in nature. Here the hierarchy of controls should be utilized to prioritize which actions should be completed to yield the most effective deterrent to future failures. Thus, for this example appropriate corrective actions would be:
This method is useful for a variety of incidents, but will only be effective if the initial post accident investigation is conducted thoroughly and with all of the people involved in the incident communicating pre-incident conditions without fear of reprisal or discipline. The typical management stance of “Blame the worker” will yield ineffective corrective actions like more training, more work rules and multiple layers of oversight. I advocate the "Learning meeting" approach described in Dr. Todd Conklin's books. Instead of building a timeline of cause and effect data, start from the beginning of the affected employee's day, ask what the work conditions were like, had they done the job before (i.e. what went right all of the times before it went wrong during this incident?) and surface all of the contributing factors that resulted in the incident. Utilize technical resources, co-workers and supervisors to bring their perspectives. And guide the process to yield the most information, the deepest learning and true understanding of how the task is actually done. Although the majority of accidents are initiated by an action by an employee, not investigating further and determining why the employee thought taking such action would yield a positive result rather than the negative one that actually happened will shed light on how the work is actually done at the company rather than how management or the Safety depratment thinks it is being done. Studies show that this deviation (usually unseen by management) is where most incidents spring from. 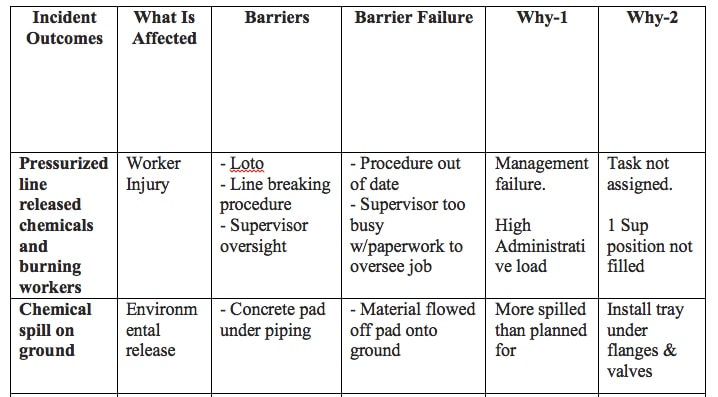  I recently read an article that was an update about a legal case proceeding from a trench collapse and double-fatality that happened in the Boston area in 2016. Kelvin “Chuck” Mattocks, 53, a married father of six, and Robert Higgins, 47, were both killed on Oct. 21, 2016, while they were helping to install a water and sewer pipe for an apartment building in South Boston. The workers drowned in a twelve-foot deep, un-shored trench, when the soil under a fire hydrant collapsed and the pipe supplying it broke. Both men were trapped by mud and debris and drowned when water filled the trench. The company was charged with eighteen willful, repeat and serious violations of workplace safety standards and issued a fine of $1,475,813. The company owner, who was supervising the work when the trench collapsed, was criminally charged with manslaughter due to numerous willful violations of OSHA’s Subpart P Construction Safety Standards for Excavation and protective systems. Among the violations cited were failure to provide shoring or a trench box, lack of worker training, lack of a ladder to exit the trench, and not providing hardhats and safety glasses to the workers. A review of the OSHA requirements yields the following safeguards which were required to have been in place for this work (Keep in mind this was a 12ft deep trench in an urban area.):
Subsequently, the owner’s defense lawyers filed doctored training sign-in sheets in an attempt to “prove” that the workers deliberately ignored safety rules. The fraudulent records were not accepted into evidence. The OSHA excavation safety standard was published in 1989, and the hazards of working in unprotected trenches are well documented and known to most companies and workers in the construction industry, and yet accidents and injuries continue happening in trenches. There were more trench fatalities in 2016 than in 2014 and 2015 combined (see graphic)! Although the most serious and potentially fatal incidents involve trench cave-ins and engulfment by loose material, there are numerous other hazards that can cause injury. Falls in and around trenches and excavations can cause broken bones and impalement. Falling debris or overhead loads, atmospheric hazards and adjacent mobile equipment can also injure construction workers and tradesmen. Work sites involving trenching and excavation tend to be dynamic, quickly changing operations where hazard recognition and control requires continuous attention. This explains how many accidents occur since the “work-as-planned” rarely matches the “work-as-it is-really-done” as the job evolves. Encountering unstable soils, having to dig deeper to locate utilities, using obsolete or inaccurate drawings, etc. can radically alter the scope of work in the field. When this happens, well trained employees, lead workers and superintendents need to step back and draw on the basic principles of trench safety: Are we digging deeper than 5 feet? Is the soil stable? Do we need shoring or a trench box? Is the shoring/protective device adequate? Do workers have adequate means of egress? Is the spoils pile far enough away from the edge of the trench, is it a hazard? What other hazards are in and around the excavation or might develop over time? The truly “competent person” will make decisions based not just on getting the work done, but on how to get the work done Safely. The OSHA excavation safety standard was published in 1989, and the hazards of working in unprotected trenches are well documented and known to most companies and workers in the construction industry, and yet accidents and injuries continue happening in trenches. There were more trench fatalities in 2016 than in 2014 and 2015 combined (see graphic)! Although the most serious and potentially fatal incidents involve trench cave-ins and engulfment by loose material, there are numerous other hazards that can cause injury. Falls in and around trenches and excavations can cause broken bones and impalement. Falling debris or overhead loads, atmospheric hazards and adjacent mobile equipment can also injure construction workers and tradesmen. Work sites involving trenching and excavation tend to be dynamic, quickly changing operations where hazard recognition and control requires continuous attention. This explains how many accidents occur since the “work-as-planned” rarely matches the “work-as-it is-really-done” as the job evolves. Encountering unstable soils, having to dig deeper to locate utilities, using obsolete or inaccurate drawings, etc. can radically alter the scope of work in the field. When this happens, well trained employees, lead workers and superintendents need to step back and draw on the basic principles of trench safety: Are we digging deeper than 5 feet? Is the soil stable? Do we need shoring or a trench box? Is the shoring/protective device adequate? Do workers have adequate means of egress? Is the spoils pile far enough away from the edge of the trench, is it a hazard? What other hazards are in and around the excavation or might develop over time? The truly “competent person” will make decisions based not just on getting the work done, but on how to get the work done Safely. |

Dave Paoletta:I've always been more interested in what the worker has to say about Safety than what the manager or Safety person thinks... Archives
March 2020
Categories |
 RSS Feed
RSS Feed